


CASE OF THE WEEK – “Fibrous Dysplasia of the Clivus skull bone” by Dr Shekhar Shikare, HOD & Consultant, Nuclear Medicine, NMC Royal Hospital Sharjah (RADIONUCLIDE BONE SCINTIGRAPHY)
The incremental value of RADIONUCLIDE BONE SCINTIGRAPHY in fibrous dysplasia of bone
Introduction
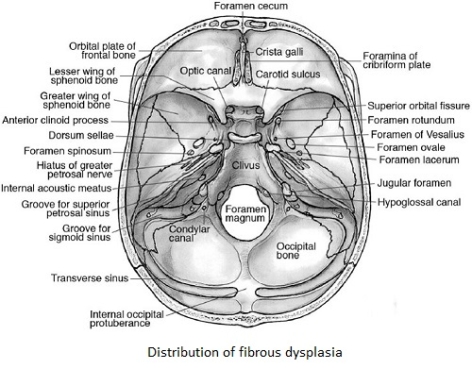
Fibrous dysplasia (FD) is a developmental disorder caused by abnormal proliferation of fibroblasts resulting in replacement of normal cancellous bone by structurally weak, immature osseous tissue. This process of unknown etiology, which mainly affects the younger population, may be monostotic, polyostotic or associated with McCune-Albright syndrome. The monostotic FD usually involves the temporal bone, orbit, mandible, and paranasal sinuses in craniofacial region.
Fibrous dysplasia (FD) of the isolated clivus, first described by Lichetenstein in 1938, is a very rare developmental, non heridtory disorder by abnormal proliferation of maturation of fibroblast resulting in replacement of the mature bone by weak and immature bone.
FD might be confused with other disease involving the clivus, for which a more aggressive surgical approach is generally advised. Furthermore, with advancement and wide use of computed tomography (CT) and Magnetic resonance (MR) imaging, many of clival FD can be detected incidentally. The awareness of and differentiating it from other skull base lesions is central in managing the patients with FD in the clivus.
Case
33 years old lady with history of increased frequency of sharp headache attacks up to four times per month mainly in left temporal side associated with nausea and mild dizziness. Sometime with prior vision disturbance but as well vision disturbances without following headache since six month have been further clarified.
X-ray skull showed increased sclerosis in the region of clivus, MRI brain with contrast revealed a contrast enhancing mass at left clivus, which likely the reason for her complaints and a white matter lesion in left frontal on unknown origin.
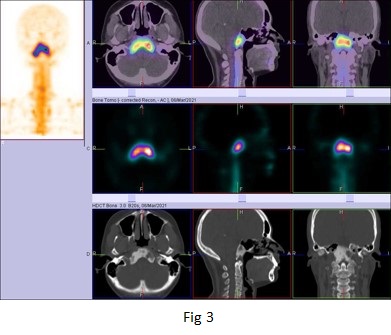
CT Scan Images
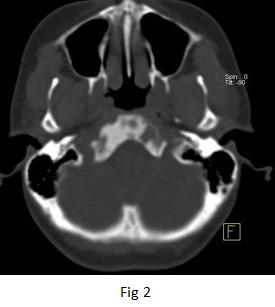
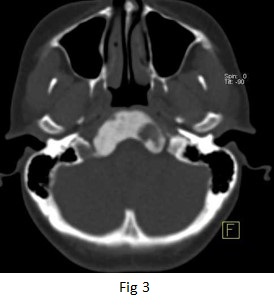
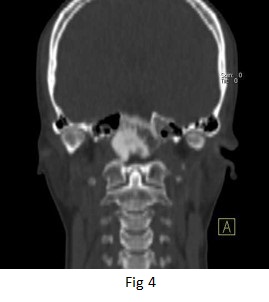
The clivus skull bone shows an expansile sclerotic appearance lesion with ground glass density pattern & scattered areas of radiolucency.
There is no cortical destruction or soft tissue component, boundaries of the sphenoid sinus, foramen magnum and adjacent bone of the skull base are uninvolved favors fibrous dysplasia.

CT SCAN images of skull (figure 1 to 5)
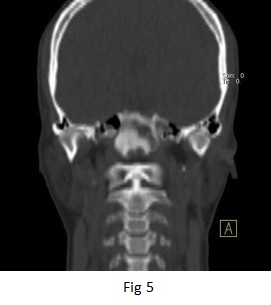
Referred for 99mTc MDP whole body bone and SPECT CT scintigraphy to evaluate if it is MONOSTOTIC or POLYSTOTIC fibrous dysplasia.
99mTc- MDP WHOLE BODY BONE AND SPECT-CT FUSED IMAGES OF SKULL confirms that involvement is confined to the clivus without evidence of disseminated disease. There is intensely increased uptake in CLIVUS BONE OF THE SKULL. ( figure 1 to 5).
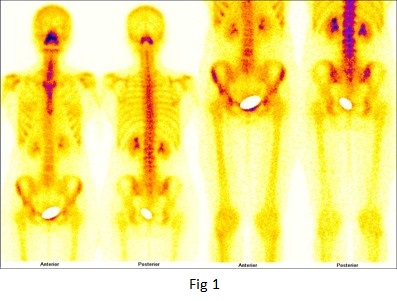
99mTc MDP whole body and spot images of skull bones (figure 1 & 2)
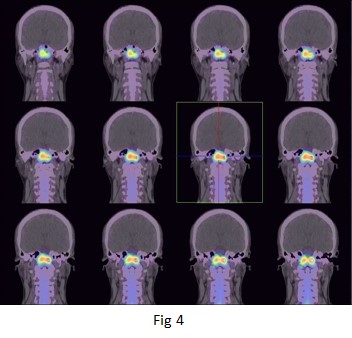
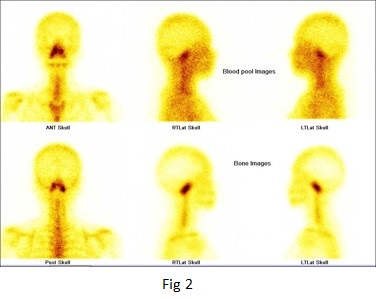
99mTc MDP SPECT-CT images of skull bones (figure 3 & 4)
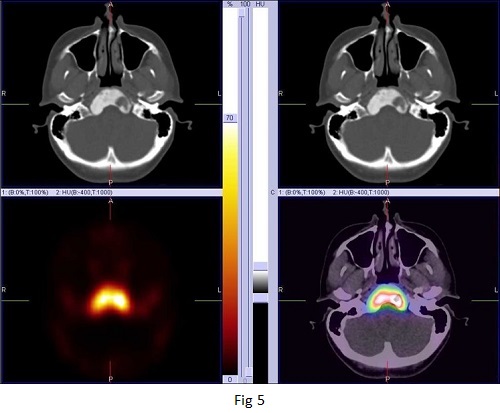
99mTc MDP SPECT-CT images of skull bones (figure 5)
Discussion
In 70% of cases FD affects a single bone, Monostotic FD, with the frontal, sphenoid, ethmoid, orbit, zygoma, maxilla, mandible, and temporal bones being the common sites affected in craniofacial bones. However, monostotic fibrous dysplasia of the clivus is extremely rare. In 30% of cases FD is polyostotic affecting several bones, where the craniofacial bones are mainly affected.
FD of the Clivus can be present with headache but in severe cases cranial nerve involvement may occur. Literature stated the diagnosis is generally clear after a proper radiological and scintigraphic workup.
CT SCAN skull images shows the characteristic appearance of thinning of the cortical bone, expansion of the affected area with “ground glass” density.
expansion of the involved bone with intact cortical outline, along with a varied degree of contrast enhancement within the lesion and not along the adjacent thickened dura.
Radionuclide bone scans are of certain value in the diagnosis of FD and useful in determining the extent of the skeletal involvement especially in polyostotic lesions. The diagnostic specificity of FD with radionuclide bone scanning can be improved in association with other imaging modalities such as X-rays. CT scan with contrast, SPECT-CT enhances sensitivity for lesions detection over planar bone scintigraphy. In addition to improve anatomic localization of scintigraphic findings, this equipment offers the opportunity to add true diagnostic information derived from CT imaging.
However, biopsy might be needed if the diagnosis is doubtful or malignant transformation is suspected.