CASE OF THE WEEK – “Gastric Cancer Presenting as Gastric outlet obstruction and misdiagnosed as duodenal ulcer” Dr. Ali Al Ghrebawi, HOD & Consultant, General Surgery, NMC Royal Hospital Sharjah
Gastric Cancer Presenting as Gastric outlet obstruction and misdiagnosed as duodenal ulcer
A 40-year-old male presented to us with the clinical signs and symptoms of gastric outlet obstruction. The patient has been operated twice before and was diagnosed as perforated duodenal ulcer, first operation was laparoscopic operation second operation was laparotomy because of sepsis and peritonitis. In his past history he has got two gastroscopies and two abdominal CT scans done within one month starting from the 25th of January 2021, till the time he presented to us in the mid-February.
In all these gastroscopies, abdominal CT scans, last two operations and all the pathological reports what he presented to us everything shows that he has a perforated duodenal ulcer. We have done the routine preoperative diagnosis through doing gastroscopy, done by Dr. Piyush, showing gastric outlet obstruction, small ulcer in the peptic region and thickening of the wall, then we have done abdominal CT scan. Abdominal CT scan, shows gastric outlet obstruction, thickening of the pylorus and duodenal wall with no peri-gastric enlarge lymph nodes, no signs or any pathological findings suggestive of cancer.
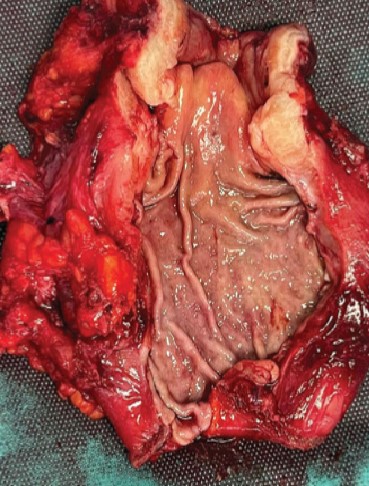
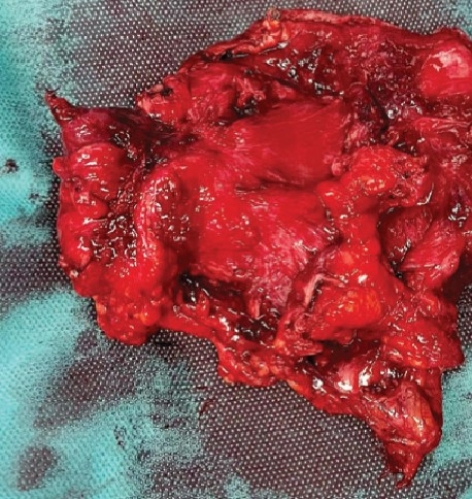
According to these diagnoses we made the operation, it was Laparotomy and Billroth type II operation with gastrojejunostomy Roux-en-Y, done successfully with no complications and patient was discharged at the 3rd post-operative day. The pathological report came out to be a Gastric cancer involving 8 of 10 Lymph nodes. Gastric adenocarcinoma moderately differentiated (9.0 x 5.5 x 2.2 cm), diffuse type and tumor invades through the muscularis propria into the subserosal connective tissue and undermine duodenal mucosa, 8 of 10 regional lymph nodes show metastatic carcinoma.
This has been discussed in our MDT tumor board and the decision was made to first do PET CT scan for the patient and then if there is no any signs of still having cancer in the body, we will do the curative three cycles chemotherapy and then after the chemotherapy we will do again a re-evaluation and again a new PET CT scan, and if still no signs of having cancer the next step will be again either chemotherapy or new surgical options to be discussed. The PET CT done and shows no weiter pathological malignant findings .which give the patient the curative therapy option