


CASE OF THE WEEK – “Use of Sentinel Node Lymphoscintigraphy in lower lip intra oral acinic cell carcinoma (unusual) & Gamma Probe Guided Sentinel Lymph Node Biopsy (SNB) ” by Dr Shekhar Shikare, HOD & Consultant, Nuclear Medicine, NMC Royal Hospital Sharjah
Introduction
Acinic cell carcinoma represents a well-established, although uncommon, entity in the classification of neoplasms of salivary gland origin. The parotid salivary gland is the most frequent site of acinic cell carcinoma, whereas the lip is a particularly unusual site.
Oral cancer is responsible for 200,000–350,000 cancer-associated fatalities per year worldwide and is thus ranked sixth about the cause of mortality due to tumors. Beside the time of diagnosis and the consequent size of the tumor, the presence of lymph node metastasis in the neck is the most important prognostic indicator.
The combination of pre-operative lymphoscintigraphy and the intraoperative detection of the SLN with a Gamma probe allows the radioactive tracer in the lymph nodes to be precisely located during the surgery.
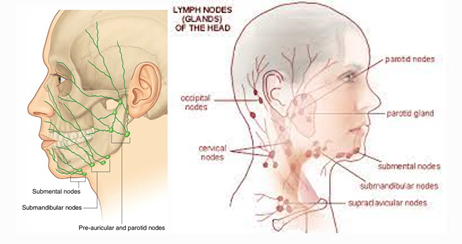
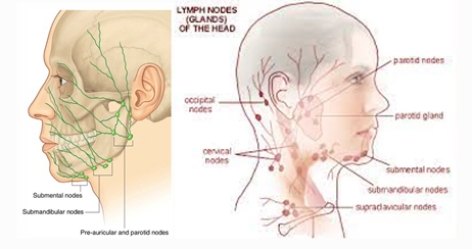
Lymphatic drianage of the lower lip Case
54 years old lady with history of small intra oral lower lip swelling since last couple of months
Biopsy shows acinic cell carcinoma (the tumor shows low grade appeareance with predominant features of intercalated duct type cellular differentiation.
On balance a classification of acinic cell carcinoma is maed, with some features of epithelial myoepithelial carcinoma also present)
99m Tc – Nano colloid SENTINEL LYMPH NODE SCINTIGRAPHY
Procedure: Tracer injection around the left lower lip lesion intra oral & subsequently at 60 minutes (Static and SPECT-CT fused images) are obtained. (figure 1 & 2)
FINDINGS
It shows SLN in submental region (more so towards right side from the mid line) as appreciated in Static (figure 1) & Hybrid SPECT-CT images (figure 3)
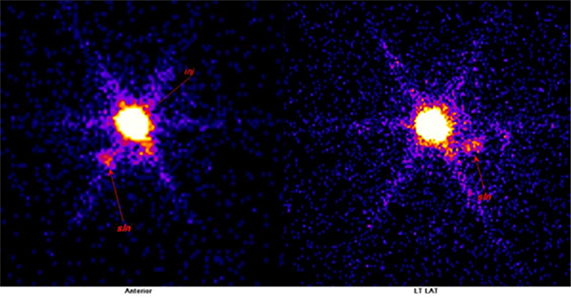
Figure 1 (static)
99mTc-Nano Colloid Sentinel Lymph Node Images Showing Sln As Shown With Arrow
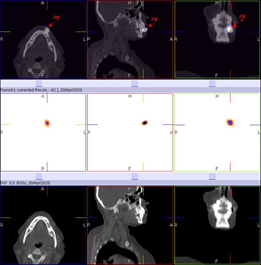
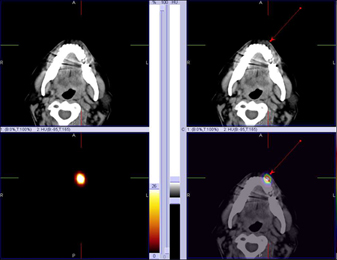
Figure 2
99mTc-Nano colloid Hybrid SPECT CT image showing injection site of the tumor. (as shown with arrow)
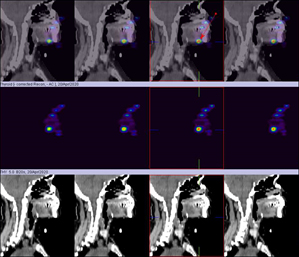
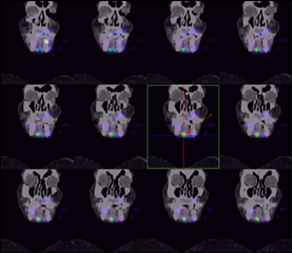
Figure 3
99mTc-Nano colloid Hybrid SPECT CT image showing SLN in submental region (as shown with arrow)
Patient underwent Gamma probe guided submental SLN removal. SNB specimen shows negative for metastatic deposit.
Discussion
The concept of an SLN biopsy provides the possibility of accurate pathological cervical node staging, whilst minimizing the invasiveness of the procedure and its associated morbidity. In addition, pre-operative lymphoscintigraphy and intraoperative detection with a hand-held Gamma-probe have the additional advantage of identifying aberrant drainage pathways.
The SLN biopsy has the benefit of concentrating only on the relevant nodes for pathological examination. This selection allows a more in-depth evaluation of the small number of sentinel nodes, using step serial sections and immunohistochemistry. However, if there are multiple SLNS at different levels, the number of SLNs that should be removed for the examination remains unknown. Most studies recommend the removal of at least 2–3 SLNs to reduce the possibility of false-negative results.